
By Ion de Andrade
If Covid’s deaths were concentrated in childhood, strong measures would have already been established internationally, in Brazil and in each state of the federation to protect the lives of children.
In the booklets and booklets that would exist everywhere and in countless versions, it would be advisable that the utensils for use by children should be separated from those of the family; that everyone wore masks to relate to them; that your meal schedule should be theirs alone; that, having space, the families reserved them primarily for the children to spend the day, which would contribute to keep the distance from the rest of the family.
Their symptoms would be followed with great zeal by the health teams, in WhatsApp groups of Primary Care and in regular home visits, health agents would be guided to a real surveillance war and would join it with enthusiasm; monitoring and health education would be done with determination and determination and positive cases would be identified early and would receive immediately from the first treatments.
This is the set of measures that should be recommended for the protection of the elderly!
The fact that mortality by Covid-19 is concentrated among the elderly, unfortunately, is accompanied by a kind of naturalization of deaths, which then become invisible, making it extremely difficult to manage the epidemic and ceasing to be the object of any specific policy.
However, the participation of the elderly in mortality insists on corresponding to a number that is between 70 and 90% of the total in Brazil, and this is also the age group that most burdens health services and that takes the longest hospitalizations.
In Rio Grande do Norte, these considerations have been considered since the beginning of Social Isolation.
What do these percentages mean mathematically in the pandemic?
The elderly in Brazil, correspond to about 12 to 14% of our population, but represent 70 to 90% of deaths by COVID. Each percentage point of the protected elderly population would impact a reduction of 5% to 6% in mortality and 4 to 5% of hospitalizations.
If we could, by an absurd hypothesis, uproot the elderly from the epidemic, we would be solving 70 to 90% of deaths and more than half of hospital admissions, the longest, the most expensive and the least capable of saving lives. In Brazil today, the 7321 deaths would be reduced to 2196. If we consider ten hospitalizations for death, we would have saved 51,250 hospitalizations across the country in this first long month of the epidemic.
This hypothesis, of the total withdrawal of the elderly from the epidemic is entirely absurd, but what would be the viable hypothesis in terms of the percentage of protection of the elderly population?
Although we do not know, because our Public Health strategy has been reduced to “Stay at Home”, we can estimate to what extent we could reduce hospitalizations and deaths with a policy focused on protecting the elderly from contagion.
Let’s look at parts:
If I have 100 deaths, of which 25% occur in people under the age of 60, it means that 75 deaths will occur in the population aged 60 and over.
If we reduce this percentage of elderly people to 60% with preventive policies instead of 75% (which seems possible) this would mean that in this case there would be 40 deaths of people under 60 in this hypothetical new group of 100 deaths. This apparent increase in the number of people under 60 is only proportional, they would still be 25% of a greater number of deaths that, in this case would not have occurred, due to the active measures to protect the elderly from contagion that in this example would have reduced deaths in the elderly from 75% to 60% of the total.
Now, these 40 deaths that occurred at ages below 60 years old, are therefore 25% of a total of 160 deaths. This means that by reducing the presence of elderly people in mortality by 15 points (from 75% to 60% of the total), we would have saved 60 lives in each group of 100 deaths and would have stopped hospitalizing, in that proportion of ten hospitalizations for one death , 600 patients, 120 of which are severe.
If all of this is true, what is going on?
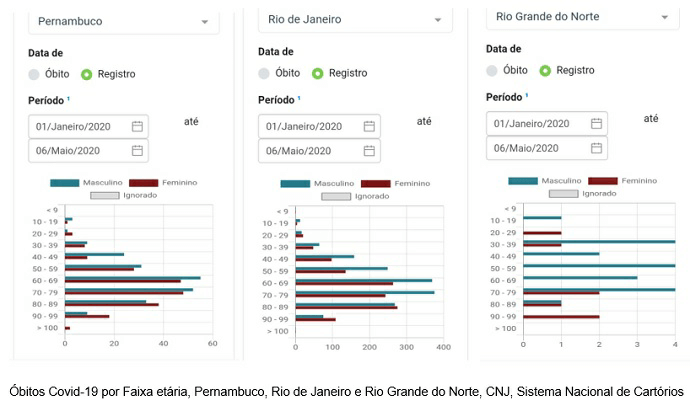
The graphs below show the atypia of Rio Grande do Norte in relation to the other states.
It is obvious that, in terms of Public Health, specific policies to protect the elderly should have been or are being implemented in a complementary way to Social Isolation.
But it is not what we see.
What we see is that, besides “Stay at home” and the respiratory etiquette, there is little and not only in Brazil, in terms of guiding families on how to prevent their elderly from being infected by Covid, from dying and before that occupy a hospital bed for 15 days, contributing to what has been called the collapse of the health system.
There are countries that are simply proposing to the elderly declarations of renouncing intensive care, so that their “inevitable” deaths will not occupy the bed of someone younger who could be saved long and uselessly.
This macabre logic, which is being naturalized, is the “ethical” complement to the previous abandonment of COVID prevention among the elderly and means that neither Public Health protects the elderly, nor the elderly should wish to stay alive.
Now, with less mobility than the young person, the elderly are essentially contaminated at home, in the dynamics of Social Isolation itself, which is not 100% safe and would be much worse without it. It is in this environment (the house) that “Stay at Home” established as insurance that the elderly person will acquire the COVID from a member of their family, who, unfortunately, was contaminated on the street, by solving the inevitable domestic problems (purchases and payments) that continue to require people to leave.
This younger relative will get sick. Statistically speaking he will have a good chance of developing mild symptoms or being asymptomatic. The elderly, however, will die, not before having crossed a hospital ordeal where they can spend 15 days intubated …
The naturalization and invisibility of the death of the elderly, socially involuntary, but wrong and the result of a deep-seated prejudice that now shows how deep it is, throws us into a trap that harms society as a whole.
Specific measures to protect the elderly in the context of households should therefore be encouraged in each family nucleus where an elderly person lives.
These measures must be supported by the Public Power and by the communities, which should also be encouraged to create networks of solidarity with those elderly people who live alone or with their elderly spouse.
These elderly people must be the object of everyone’s attention so that they do not have to go out into the streets to make their purchases or payments.
The role of State and Municipal Health Departments, Primary Care and Community Health Agents is crucial in this task of monitoring suspects and cases, fostering neighborhood solidarity and educating the community on health.
Rio Grande do Norte
In Rio Grande do Norte, a number of initiatives have been pointing in this direction.
With institutional support from the Laboratory of Technological Innovation in Health (LAIS / URN) coordinated by professor Ricardo Valentim and the State Secretariat of Public Health (SESAP / RN), directed by dr. Cipriano Maia de Vasconcelos, the elderly protection agenda has been occupying, since mid-March, time on radio and TV.
The Expert Advisory Committee appointed by SESAP to confront COVID considered, even in its last opinion, that this policy is one of the justifications, together with the early decree of Social Isolation, by Governor Fátima Bezerra, for the eased curve that the state has been observing so far.
A booklet (click here to obtain and replicate it) aimed at the work of Community Health Agents and the guidance of families with the elderly was edited and published with the support of Civil Society (the RN Solidariedade COVID group, coordinated by the Engineer Hermínio Brito) and the Public Ministry, the Elderly and Health, coordinated respectively by dr. Suely Magna de Carvalho and by dr. Raquel de Ataíde Fagundes, recommended for Natal a striking action of Primary Care in the visit and registration of families with elderly people, to ensure the protection of the contagion of these elderly people at home (click here to know the recommendation of the Public Ministry)
An application, Orientacorona, (click here to know) developed by the team of Professor Lyane Ramalho at UFRN was created and included among its guidelines the home protection of the elderly from contagion.
The Department of Social Communication at UFRN, together with the LAIS Communication Department through the teams of professors Lilian Muneiro, Valéria Credídio and professor Juciano Lacerda not only created abundant educational material, spots (click here to know) and images, as it has a continuous effort was made to project this idea of protecting the elderly from contagion in all media.
Simultaneously teachers Nadja Rocha, Vilani Nunes, Paulo Rocha, Kenio de Lima, Severina Alice Uchoa, Lyane Ramalho, in addition to myself and with the collaboration of Professor Massimo Giangaspero, we elaborated the bases of this policy for Primary Care in a document already published in GGN (click here to read). The Revista Brasileira de Geriatria e Gerontologia also published an editorial summarizing this elaborated Policy (click here to read).
How are the numbers in Rio Grande do Norte?
We know that the fight against the pandemic has to be won every day and that it is nowhere to be won, which includes Rio Grande do Norte. In the epidemic process that is developing in the state, we are currently challenged by a change in the profile of those confirmed, which now includes people from popular neighborhoods and the interior of the state, in addition to the middle sectors that are still immersed in the epidemic. It is in these new environments that these policies for the protection of the elderly will have to be consolidated, which will require hard work.
For all these reasons, we know that our numbers may change, but today the elderly correspond to 55.88% of the total of 68 deaths registered in the state.
When we know that in Italy they corresponded to 96% of the total, in China to 85%, in Spain to 90% and in the Northeast to an average of 70%, we can measure the meaning of the brand achieved by Rio Grande do Norte, which had courage and energy to develop and apply its own policy to face the pandemic that it dared to add to “Stay at Home” the “Protection of the Elderly” at home.
This may have meant, as we believe, an equal or greater number of 32 lives saved and 320 hospitalizations that did not occur, considering ten hospitalizations for death, of which 64 were serious.
We bring our report so that decision makers in Brazil everywhere add to “Stay at Home” the idea of protecting the elderly at home in the context of Social Isolation.
If we naturalize the deaths of the elderly and do not take specific initiatives, the results of the pandemic will be much worse than they could be.
There is work for everyone, State and Municipal Health Departments, Universities, Public Ministry and Civil Society.
The material we produce is free to use, the application, the Primer, the advertising spots can be used at will. Others can be worked out.
Good job to those who understand and adhere!
Ion de Andrade is an epidemiologist physician at the State Department of Public Health, SESAP / RN / CEFOPE / ETSUS and researcher at the Laboratory of Technological Innovation in Health, LAIS / UFRN




